28year old male with complaints of SOB,pedal edema and abdominal distension
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case I have seen
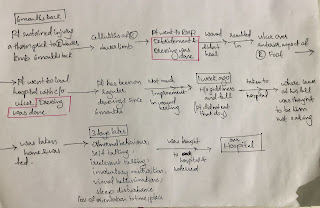
28 year old man, came to opd on 5 dec 2020 with c/o sob since 3 days already a known case of hypertensive since 12 months,ckd on mhd , non diabetic, non alcoholic, non smoker, unmarried, constructor worker from Nalgonda who was apparently alright, busy working daily at construction sites one day an year back developed high grade fever along with body pains for which he was taken to a RMP and he was given ' tablets for fever ' as the attendant describes it, which got subsided temporarily. By night he again developed fever for which he was taken to Nalgonda Hospital and was admitted for a few days and was discharged.
Since then he was on regular NSAID use for fever and body pains.
After 4months he again developed fever and he was taken to NIMS where they performed a Renal biopsy and told them his kidneys got affected because of overuse of painkillers.
Biopsy report


2 months later he developed Dyspnea at rest, reduced urine output, non productive cough, he developed even pedal edema which slowly crawled up to his abdomen cause its distension along with facial puffiness. Upon examination they were told that he had hypertension and was started on antihypertensives and that he needed hemodialysis.
During his stay in the hospital a pleural tap was done and his sputum cultures were sent too. They were negative for tuberculosis.
On examination, pallor is present

flat nails are present
Jvp raised
PR - 92 bpm, regular
Bp - 120/80 mmhg
Afebrile
chest wall retraction are present with a respiratory rate of 20 cpm
Abdomen is distended and umbilicus is everted
flat nails are present
Jvp raised
PR - 92 bpm, regular
Bp - 120/80 mmhg
Afebrile
chest wall retraction are present with a respiratory rate of 20 cpm
Abdomen is distended and umbilicus is everted


Investigations:













Treatment-
Renal transplant was asked for,for which his mother was screened and her DTPA renogram report was

Criteria for transplantation:





Treatment:
- Inj. Lasix 40 mg /iv/tid
- Tab nicardia 20 mg qid
- Tab arkamine 0.1 mg qid
- Tab nodosis 500 mg bd
- Tab shelfal po bd
- Tab metxl 50 mg bd
- Inj pan 40 mg iv od
- Tab dolo 650 mg po tid
- Tab alpha d3 po od
- Syp ascoril 10 ml
- Till 2/1/21 he was on
- T.MET XL 50mg PO/TID
- T.NICARDIA 20mg PO/QID
- T.ARKAMINE 0.1mg PO/QID
- T.LASIX 40mg PO/TID
- FROM 3/1/21 he was on
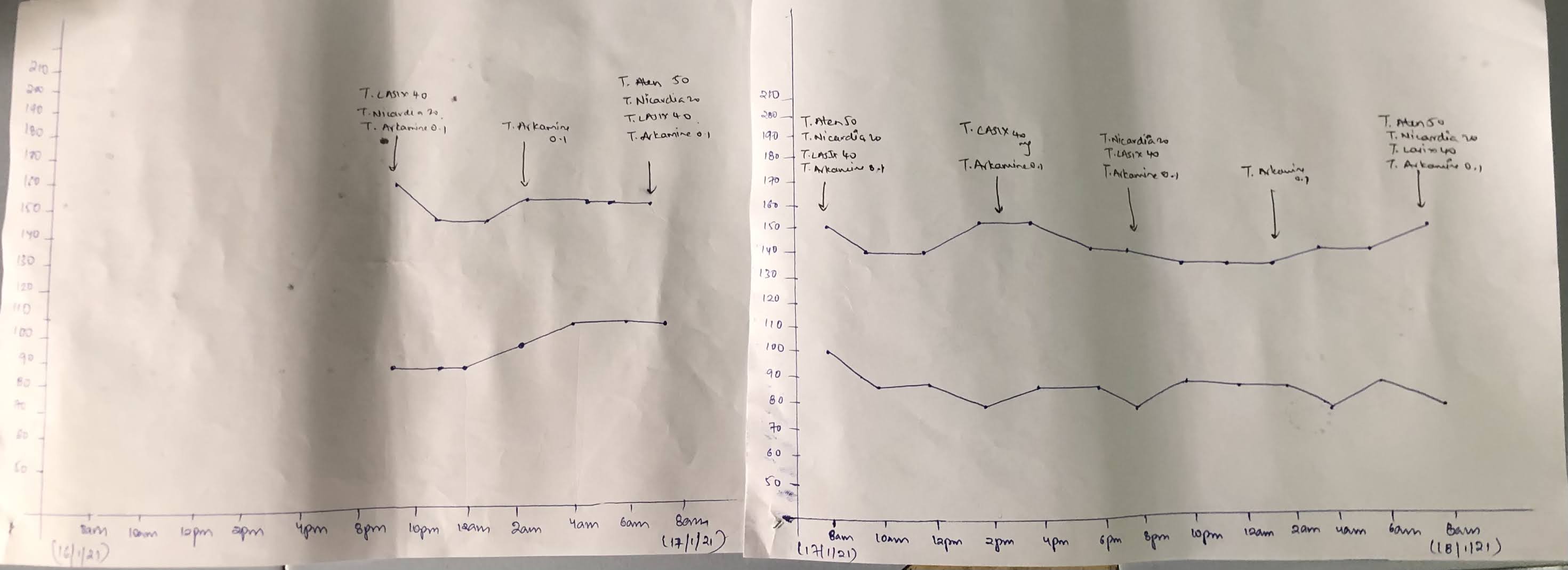
- T.ATEN 50mg PO/OD
- T.NICARDIA 20mg PO/QID
- T.ARKAMINE 0.1mg PO/QID
- T.LASIX 40mg PO/TID
Bp monitoring-


Comments
Post a Comment